
")
Lung tissue
Open and thoracoscopic lung biopsy
There are 3 different techniques for a lung biopsy, the transbronchial, the open or thoracoscopic lung biopsy and the transthoracal CT or ultrasound guided lung biopsy. Useful for the diagnostic of suspected interstitial lung disease are only open and thoracoscopic lung biopsies.
Indication and planning
- Always when the diagnostic process is not advancing anymore and the lung disease is significant and unclear or even progressing, a histopathological analysis of lung tissue is indicated
- Unclear diffuse interstitial, infectious or neoplastic process of the lung
- It is important to make a lung biopsy early on in progressing lung disease
- You have to make absolutely sure, that the biopsy will be processed, used and interpreted in an optimal way
- For this each and every lung biopsy should be included into the Kids Lung Register
- The lund biopsy should be performed in experienced centers because of the complex sample processing and logistics
Relative contra-indications
- Radiological indication for diffuse, endstage lung disease, e. g. lung without areas of mild disease affection
- Severe cardiovascular disease, severe pulmonary dysfunction or other general risk factors for general anesthesia or surgery
- High risk, that sufficiently large biopsies from different sites (usually two different lobes) cannot be obtained
- Mechanical ventilation and immunosuppressive therapy increase the risk and the complication rate
Complications
- Risk depends on general condition and particularly the pulmonary condition
- Therefore lung biopsies should not be conducted too late
- Pneumothorax, hemorrhage, wound infection
- Prolonged intubation, pneumonia
- Risk increases with immunosuppressive therapy and prior respiratory insufficiency
- Complication rate between 6 and 65 %
- Mortality rate between 3 and 38 % depending on the extend of the underlying disease
- Complication rate is lower with VATS
Technique
A) Open
- An experienced surgeon needs only a few minutes operation time
- Incision of 3-4 cm above the area where the biopsy shall be taken
- Most of the time lateral dorsal or ventral access way
- After opening the pleural space part of the lung is grabed with a clamp and pulled through the thoracotomy opening
- With a stapler two biopsies from two different lobes are taken
B) VATS
- The video assisted thoracoscopic surgical biopsy (VATS) is done under general anesthesia and endotracheal intubation
- One-sided lung ventilation is necessary and taking the biopsy migh be complicated if the lung does not collaps or has multiple adhesions
- Transthoracal trocars, one for the campera and one for the stapler and usually a third one for taking the biopsy, are inserted
- The access port can be varied depending on the lung pathology
- Shorter duration of pleural drainage, if any
- Shorter length of hospital stay
- Better cosmetic outcome
Sample processing
- The physician ordering the lung biopsy should personally receive it in the theatre and process it
- Since a lung biopsy is usually performed only once in a life time of a patient the gain of information should always be maximized. Therefore it is advisable to have a lung biopsy done in a center which is very experienced in obtaining and processing lung biopsies
- To take biopsies from 2 lobes is usefull and necessary
- Avoide the tips of the lobes and the lingula, since there are often found non specific fibrotic lesions
- Lung tissue after lobectomy or pneumectomy can be inflated via the main bronchi using fixation solution
- The inflation can induce artefacts, e. g. by wash out of macrophages
- Swab tests for microbiology should be obtained or small pices should directly be processed (culture, PCR)
Seize of lung biopsy
- At least 1 cm of lung tissue from the pleura
- In small children at least 1 x 1 cm volume, older children and adults at least 2 x 2 cm, maximal diameter 4 cm
- Avoide plane close to pleural edge canu like biopsies, since histology is most of the time non-productive
The 4 principal ways of asservating every lung biopsy
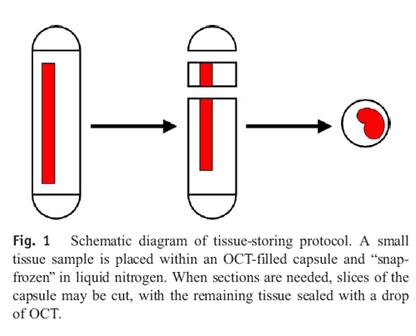
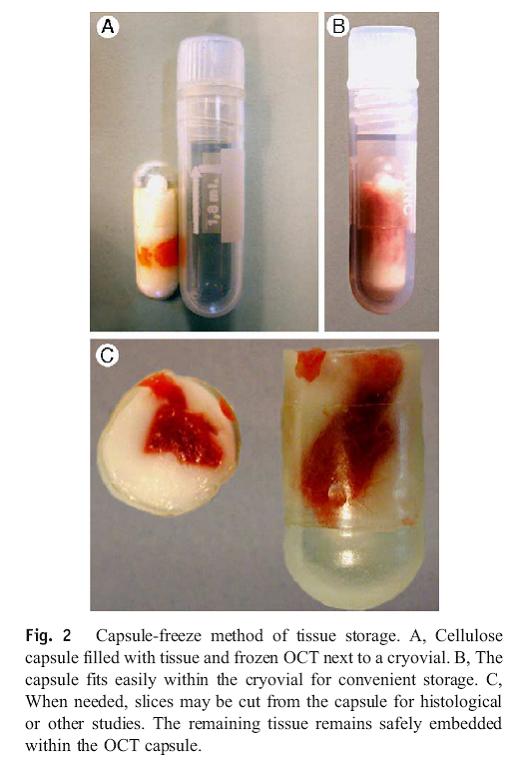
1. Freezing in OCT and liquid nitrogen
Tissue for cyro slides, immunohistology, RNA analysis, biochemical tests
- Placing the tissue sample in a cellulosis capsula which contains OCT (Optimal cutting medium). Then directly freeze in liquid nitrogen. Long term storage at – 70° C or -196° C (Lokena 2005). Technical details see below.
- Adding the tissue directly to liquid nitrogen is suitable for PCR and biochemistry. However the possibility of histopathological examinations is dispenced.
Long term storage: Transfer from liquid nitrogen (if intermediate storage is necessary place into - 80° C freezer) on dry ice and ship to the Kids Lung Register for long-term storage in a nitrogen tank.
2. Formalin fixation for conventional histology
Tissue for conventional histology
About 60-70% of the tissue blocks will be formalin fixed for conventional histology. This is done in 4% formalin.
Usually one piece is send to the local pathology and one or two other are send to the collecting point of the reference pathologists of the Kids Lung Register.
In some centers all material is shipped via the local pathology to the collecting point of the kids lung register (please use the appropriate shipping forms which can be printed in the Data Capture) or all is shipped to the collecting point of the reference pathologists at the Kids Lung Register. After sample registration an according shipping form can be found in the Data Capture Tool of the KLR.
Long term storage: Storage in formalin is only possible for a short period of time ! Therfore embedding into paraffin (= wax block) is absolutely necessary, since otherwise the tissue will be destroyed by the released formic acid. The paraffin embedding can also be perfomed by the collecting point of the reference pathologists of the Kids Lung Register.
3. Glutaraldehyde fixation for electron microscopy
Tissue for electron microscopy
Even so the tissue is not always examined by electron microscopy, a small portion without fail has to be fixed in glutaraldehyde; since storage in it is not possible for a longer peroid of time, the embedding into epoxide has to be performed; this will be done for free for allsamples by the Kids Lung Register / Institute for Pathology, Munich. Thereto 3, respectively 6 (in case of biopsy from two different locations) small pices, of about 2x2 mm are placed in glutaraldehyde. Special glutaraldehyde buffer should be used. The recipe can be found below (Fixation solution for biopsies). Alternatively aliquots of the buffer can be requested at the Kids Lung Register. The puffer needs to be stored frozen (-20°C) until used.
Long term storage: Material for the electron microscopy cannot be stored in glutaraldehyde for a longer peroid of time! It must be embedded in epoxide blocks. Alternatively, one part of the samples can be stored in glutaraldehyde buffer (like the one described above), while the other part is embedded into epoxide (service of the KLR).
Fixiation solution for biopsies (Last change: 06.05.2004)
Protocol for production:
0,4 M Hepes (FW: 238,3 in A.d. ; 238,3g – 1L – 1 Mol, 95,32g – 1L – 0,4 Mol, 9,532g – 100ml – 0,4 Mol; 4,766g – 50ml – 0,4 Mol). Adjusting pH: 7,4
- Heating 45 ml H2O at 70°C and adding 4g paraformaldehyde. This needs to be done under adding NaOH to the solution. You titrate the base until complete dissolving of the aldehyde (the solution needs to be clear). After cooling down of the solution the pH needs to be adjusted to pH of 7,4 and adding 0,4M Hepes at 100ml.
- Adding glutaraldehyde, so that the end concentration is 0,1% (400μl)
Chemicals: Aqua ad injectabilia (Braun, Melsungen, Deutschland); Hepes (Sigma,H3375), paraformaldehyde (Merck), glutaraldehyde (Sigma,G6257).
Note: The buffer is made to last 4 weeks at 4°C or 1year at –20°C, in this case prepare smaller aliqots.
4. Native for detection of pathogens
Material for microbiology
Obtain sterile microscope slides for Gram staining of the cutted surface of a biopsy. Usually three slides air dried and three alcohol fixed. Through this pathogens can quickly be identified.
Additionally under sterile conditions small pieces from the edges or left overs can be put in sterile saline for culture and PCR.
Transport
A) at room temperature (all material for microbiology, fixed for conventional histology, electronmicroscopy)
B) on-site frozen material must be shipped on dry ice (nitrogen/frozen tissue)
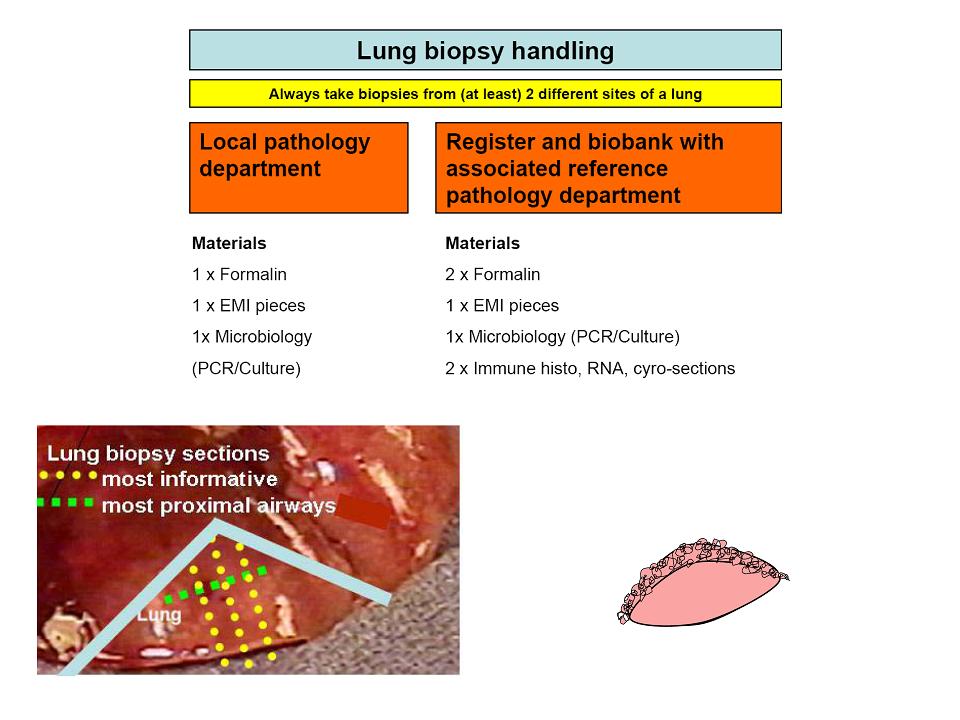
Figure 1: Material distribution of a lung biopsy in principal. Material is send to the local pathology/microbiology as well as to the Kids Lung Register. From there it is sent to the reference pathology and for asservation for electron microscopy and further special tests.
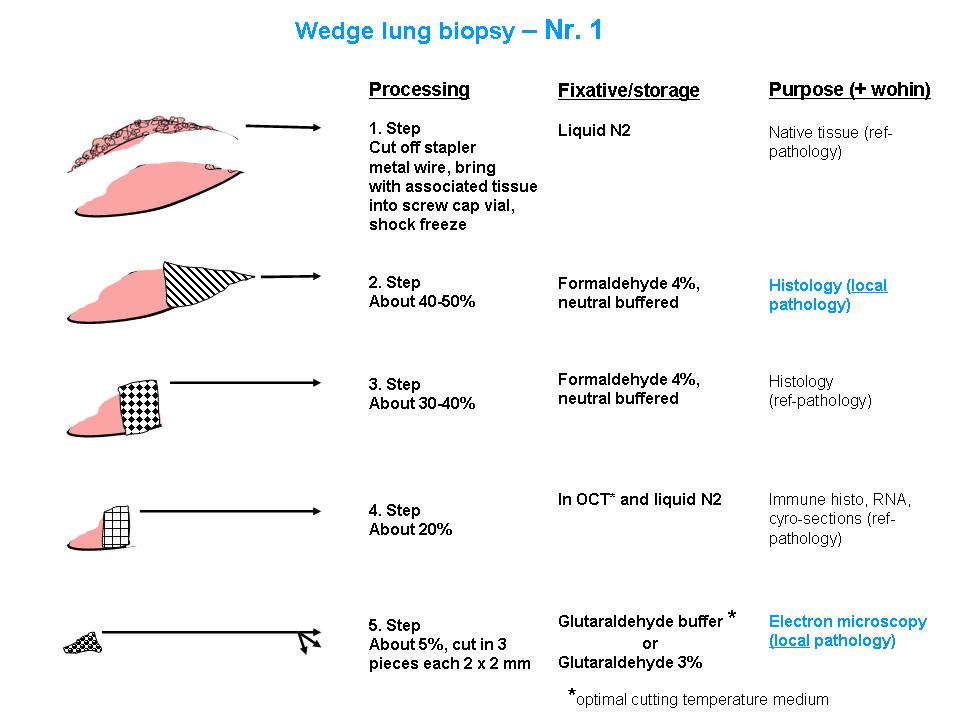
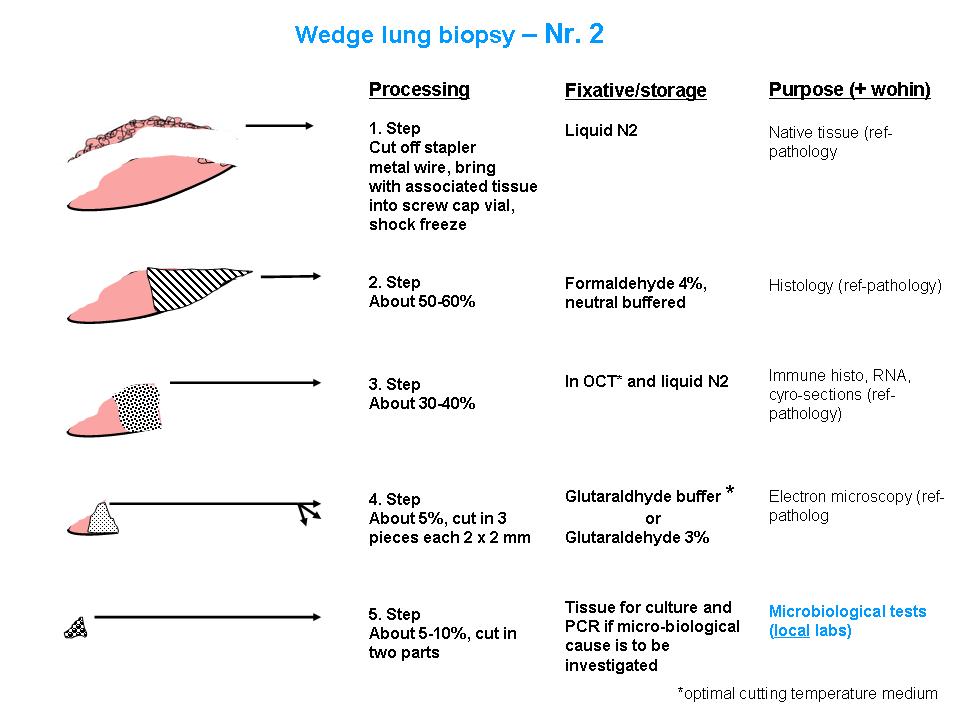
Figure 2+3: Detailed distribution of lung biopsies. Seperately displayed for two different biopsies (No. 1 and No. 2). All specifications are made in relative indication of seize.
Technical details
For correct freezing of tissue samples and for assuring further processing, the sample should be transferred into a cellulosis capsule (Nr 09262, size 00, transparent, iphas, Würselen, Germany), containing some so called cryomatrix. Cryomatrix is a medium which contains OCT (optimal cutting medium). After filling the capsule with more OCT, it is frozen in liquid nitrogen. Long term storage is possible at -70° C or -196° C (Lokena 2005).
Procedure
Working unter sterile conditions with gloves, surgical scissors or scalpel and forceps.
Cellulosis capsules (Ordering No. ), adding 1-2 drops of cryomatrix (Ordering No. OCT (Trademark)).
Placing the tissue samples in the cellulosis capsules.
Adding another 3-5 drops of cyomatrix; avoiding bubbles.
Closing the capsule and putting it into liquid nitrogen.
Afterwards transfer of the capsule into a cryovial and storing it in liquid nitrogen until final storage at -80 C, respectively shipping it on dry ice to the Biobank of the Kids Lung Register.
You should always process several small pices (ca 3 x 3 x 5 mm).
Problems
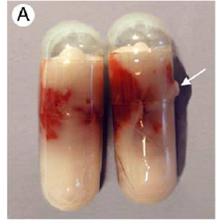
Artefacts associated with the capsule-freeze technique. One type of minor damage to gelatine capsule, showing leakage of OCT that occurred during freezing (arrow).
Furthermore link to http://epi.grants.cancer.gov/CFR/bio_fresh_tissue_app.html)
Processing of postmortal lung biopsies
Extremly important possibility; also partially for single organs, e. g. lung and liver.
Postmortal lung biopsy - a way out even for people of islamic faith! (see El-Reshaid et al, Medical Principles and Practice, 2005)
Prodcedure
Like described above, however you have to make sure, that the pices are not to big, since then they cannot be fixed well. Therefore it is better to obtain small pices (1 x 1 cm) from diffrent locations.
Native in liquid nitrogen a lot of material can be asservated.
Literature: